
If you’ve been around downhill skiing long enough, you probably know someone who has “blown out” their knee. It’s a total bummer. Usually this means someone has torn ligaments and/or meniscus tissue. The typical catastrophic “blow out” involves a full tear of the anterior cruciate ligament (ACL), which drastically reduces the passive stability of the knee required for cutting movements like turning on skis. To get back to skiing at a high level, surgical reconstruction of a torn ACL is usually requisite, though there are some “copers” that can recover most prior capacity without it. This post will focus on understanding the mechanism of non-contact skiing-related ACL injury, and how to reduce risk.
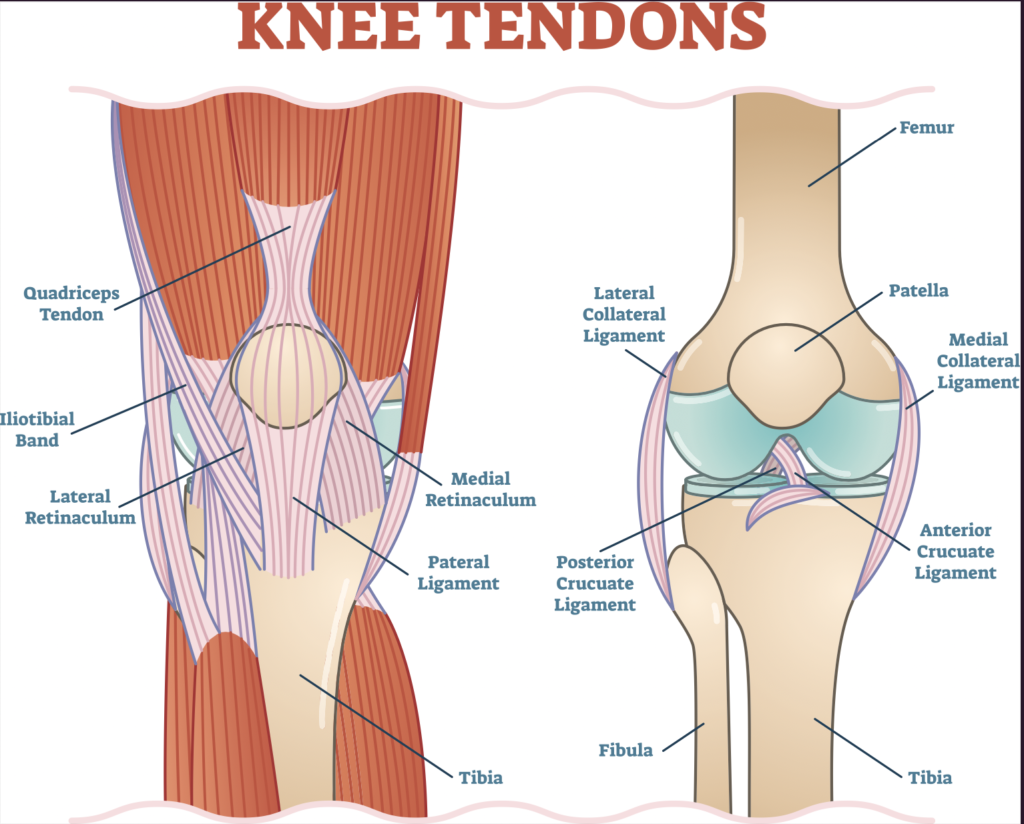
A basic understanding of knee anatomy and mechanics is useful. The knee is the connection of the shin bone (tibia) and thigh bone (femur). It mostly bends and straightens like a hinge, but it also rotates and gaps side to side a small amount. A kneecap is embedded in the quadriceps tendon to provide better leverage for the quadriceps to straighten the knee. On the backside of the thigh and knee, hamstrings connect the pelvis to the tibia, so it can bend the knee and extend the hip. Think of hamstrings like the reins on a horse and the tibia is the horse’s face. The outside hamstring turns the tibia laterally (toes out), and the inner hamstrings turn the tibia internally (toes in). Combined, the hamstring group pulls the top of the tibia back working against the forces of the quadriceps that pull it forward (remember this for later). Multiple ligaments provide passive stability to the knee. The broad and flat medial collateral ligament (MCL) resists gapping of the inside of the knee. The lateral collateral ligament (LCL) is a thick cylindrical ligament, like a pencil, resisting gapping forces on the outside of the knee. The posterior cruciate ligament primarily stabilizes posterior translation of the tibia. The focus of this article is the ACL.
Think of the ACL like a thick, strong rope inside the knee. It connects the femur to the tibia. It stops the tibia from sliding out forward under the femur and twisting to the outside. In the orthopedic world, we say that ligaments provide “passive stability.” “Active stability,” on the other hand, is provided by muscle and tendon like the quadriceps and hamstrings that can contract and relax. We will get back active stability in another paragraph.
Let’s first answer this question: “How does the ACL tear?” Think of Silly Putty. When you pull the putty apart fast, it snaps in two pieces. On the other hand, at slow speeds, it doesn’t immediately break. It just continues to stretch before slowly coming apart. Our body tissues are in a way just like Silly Putty in that they are viscoelastic. So, the mechanism of injury to the ACL, just like other tissues, involves a rapid and forceful stretch applied to the ACL. Keep in mind, the focus is on non-contact injury, so this excludes skiing into a stump or someone running into the side of your knee. The key to avoiding a tear of the ACL is to avoid knee positions and forces that pull on the ACL rapidly. More specifically, we want to avoid large magnitude, fast quadriceps contractions insufficiently stabilized by hamstring contractions AND/OR rapid twisting and gapping forces.
Therefore, the “Active Stability” system is crucial to protecting the ACL from these rapid, high load stretching forces. Training this system is how to reduce injury risk. Without going into too much detail, the “active stability” system depends on how optimized the nervous system is at responding to changes in joint and body position. Let’s just call this body awareness. Sensory information is rapidly processed to send messages to the muscles to provide joint stability. Locally at the knee and globally in terms of your body posture, all of your muscles need to be conditioned, and your body awareness needs to be finely tuned for the task. So, let’s dig into how to reduce knee injury risk.
Critical areas of focus for knee injury risk management are the following:
Optimizing balance and posture on your skis. The salient point to make is that optimizing your body position will enable better edge control, shock absorption, and promote distribution forces across the knees, hips, ankles, and trunk. The balanced position is especially critical when conditions are choppy and less predictable. For example, think of your vehicle’s suspension system adapting to a bumpy road surface. Having the appropriate bend in the lower body and trunk posture for the slope angle and speed will enable you to compress and extend like a spring through a smooth turn or absorb bumps and chatter when turning or straight lining. You must do all you can to stay out of the straight knee, hinged hips position. If you regularly ski with your upper body leaned too far forward from the hips with inadequate knee bend, the knee is in an at risk position. Studies have shown knee flexion angles of 0-40 degrees enable higher forces through the ACL when torsional stress (twisting) is applied. Torsional forces occur when turning or cutting. The “backseat” position (leaning backward) is another position that can be problematic due to the relatively high quadriceps forces required to stay upright while the hamstrings are in a disadvantaged position to provide active stabilization of the tibia (Remember, the hamstrings are your “active stability” reinforcements for the ACL). Live repetitions on skis are the best way to acquire the skills necessary for optimizing balance on your skis, but balance and posture can be trained on land too. Getting used to the ankle range of motion limitations of wearing a boot presents a unique difference in on land training versus skiing.

Quadriceps strength and fatigue resistance: From an injury prevention standpoint, a skier should have the baseline strength to perform a full squat, and they should have the fatigue resistance to hold a 90 degree wall squat for minutes. Weakness or fatigue in the quadriceps make it difficult to keep the knees bent sufficiently to avoid higher risk posture. As mentioned above, forces on the ACL during turning are greater in knee extended positions (0-40 degrees flexion).

Quadriceps to hamstring strength ratio of 50-80%: Remember, the quadriceps pull the upper end of the tibia forward, and the hamstrings pull it backward. When the quadriceps overpower the hamstrings, the ACL is at risk especially if there is a rapid load applied to the knee. These rapid loads occur frequently in choppy and variable conditions. The faster and more variable terrain a person expects to ski, the closer their strength ratio should be to 80%.
Hip strength and control of adduction and internal rotation of the femur: The knee not only bends and straightens, it also rotates and gaps medially and laterally slightly. However, the knee does not withstand twisting (torsion) and/or medial or lateral gapping forces well because there is minimal range of motion in these directions, and also poor local muscle leverage to control rotation and gapping. The gluteus maximus along with deeper rotator muscles, hamstrings, hip abductor, adductor, and flexor muscles control the femur from the top end thus influencing the alignment of the femur on bottom end (knee). Conditioning these hip muscles and training them specifically to the movements involved in skiing is crucial.
Trunk muscle control of the pelvis: The hip muscles mentioned above all attach to the pelvis, so pelvic stability is also required. In skiing, counter rotation of the trunk and the pelvis occurs to optimize alignment at any given time during turning. Therefore the abdominal muscles and trunk extensor muscles must work together to position or stabilize the “core” so the hip and thigh muscles can control the lower body and skis.
CONCLUSION: These 5 areas of focus are ways to manage modifiable risk factors. In the big picture, there are other risk factors at play including activity-specific skill and experience, body shape/architecture, and exposures to high force multidirectional activities during youth. Repeated exposures to multidirectional movements throughout a lifetime, but especially as a young person, is ideal for developing bone, tendon, and ligament strength. For young and developing bodies, this is the best injury prevention for activities later in life. However, it is never too late to get moving. Stay active and focus on building strength, balance, flexibility, and muscular and cardiovascular endurance to keep doing the things you love to do as you age.
If you’re interested in understanding your specific risk factors and addressing them through assessment and ski conditioning with a physical therapist, Iron Horse PT and Performance offers one-on-one and two person ski conditioning programming.